Article Text

Abstract
Background Non-drinkers are shown to have worse health than moderate drinkers in later life. We examine the preceding health status of non-drinkers in early adulthood, and secondly whether persistent poor health is associated with persistent non-drinking.
Methods Using two prospective British birth cohort studies established in 1958 (National Child Development Study (NCDS)) and in 1970 (British Cohort Study (BCS)), participants who reported ‘never’ or ‘never had an alcoholic drink’ to drinking status questions in successive waves from 23 to 26 years in the NCDS/BCS were derived as ‘lifetime abstainers’. Logistic regression on the odds of being a lifetime abstainer was carried out on changes in limiting long-standing illness (LLSI) in the NCDS and long-standing illness (LSI) in the BCS, adjusting for sex, education, poor psychosocial health, marital and parental status.
Results Participants with an LLSI in consecutive waves since 23 years had 4.50 times the odds of someone who did not have an LLSI of being a lifetime abstainer at 33 years (95% CI 1.99 to 10.18) and 7.02 times the odds at 42 years (2.39 to 20.66) after adjusting for all factors. Similarly, in the BCS, having an LSI in consecutive waves resulted in higher odds of being a lifetime abstainer at 30 years (OR 2.80, 1.88 to 4.18) and 34 years (OR 3.33, 2.01 to 5.53).
Conclusions Persistent LSI was associated with remaining a non-drinker across adulthood. Studies comparing the health outcomes of moderate drinkers to lifetime abstainers that do not account for pre-existing poor health may overestimate the better health outcomes from moderate alcohol consumption.
- ALCOHOL
- LONGITUDINAL STUDIES
- SOCIAL EPIDEMIOLOGY
- HEALTH BEHAVIOUR
Statistics from Altmetric.com
Introduction
Evidence for the J/U-shaped relationship between alcohol consumption and mortality and morbidity, where non-drinkers and heavy drinkers have worse health than moderate drinkers in later life, is established in the literature. While this relationship appears among diverse populations and through time1 and in various conditions such as coronary heart disease,2 cardiovascular disease,3 all-cause mortality4 and, more recently, cognitive decline,5 whether the better health outcomes of moderate drinkers compared with non-drinkers can be completely attributable to moderate alcohol consumption has been debated.
The most prominent criticism was first proposed by Shaper et al6 who argued that many non-drinkers in later life are ex-drinkers who have stopped drinking due to illness; thus, it is their pre-existing poor health which exaggerates the poor health outcomes of non-drinkers relative to drinkers. This is sometimes referred to as the ‘sick-quitter’ bias. Indeed, ex-drinkers have higher rates of doctor-diagnosed illnesses including heart disease,7 and a diagnosis of a chronic condition was found to be associated with an increase in probability of a reduction or cessation of alcohol consumption.8 ,9
However, poor health was also found to be associated with non-drinking among young adults,10 even after adjusting for a range of social and demographic factors.11 This raises the question as to whether poor health may precede non-drinking at the very onset of one's drinking trajectory and whether continued poor health is a reason for refraining from drinking across the life course. If this is the case, then the worse health of non-drinkers in later life may suffer from double bias, first, from ‘sick quitters’ and second, from those who abstain throughout life due to continual poor health indicating a further bias among lifetime abstainers. We call the latter ‘sick non-starters’. This is the subject of investigation in this study through the use of two nationally representative prospective British cohort studies to assess whether persistent poor health is associated with remaining a non-drinker from early adulthood.
Method
Survey design
The 1958 National Child Development Study (NCDS) and the 1970 British Cohort Study (BCS) are prospective cohort studies established on around 17 000 British babies born in their corresponding years. Data from the NCDS were collected when participants were aged 7, 11, 16, 23, 33, 42, 46 and 50. Similarly, data from the BCS were collected at birth and at ages 5, 10, 16, 26, 30, 34 and 38. In each cohort, data was collected from a variety of sources including parents, medical examiners and schools which covered a wide range of areas including socioeconomic status and health. We use NCDS data collected at ages 16 (1974), 23 (1981), 33 (1991) and 42 (2000), as well as BCS data collected at ages 26 (1996), 30 (2000) and 34 (2004) since drinking frequency questions were not asked at 38 years. Our reason for using two cohorts was to validate the hypothesis that persistent self-reported illness is associated with persistent non-drinking since this hypothesis has not been explored before, rather then to compare the effects between the two cohorts. The different time points and measurements used in each cohort would also make it difficult to make a direct comparison.
Measurements
Alcohol consumption
In each of the specified waves, participants were asked “How often do you usually have an alcoholic drink of any kind?” We derived a lifetime abstainer variable using a bottom-up approach by netting together all those who said “Never nowadays” or “Never had an alcoholic drink” at 23 and 33 years, and in the second model up to 42 years. The same method was applied in the BCS using “Never nowadays” or “Never had an alcoholic drink” answers from 26 to 30 years, and in the second model up to 34 years. These two options “Never nowadays” and “Never had an alcoholic drink” are provided to make a distinction between those who have never drank alcohol throughout their life. To avoid confusion, we refer to people who stated “Never nowadays” as non-drinkers and the latter as self-identified ‘lifetime abstainers’.
We also compare findings with self-identified ‘lifetime abstainers’ who are those who stated “Never had an alcoholic drink” using the BCS at 30 and 34 years. This was not carried out in the NCDS as this option was not provided at 33 years. This method of deriving lifetime abstainers from participants’ self-report is what is commonly used in the literature; however, two studies have found that half of the participants who claimed to have never drunk alcohol reported drinking in the previous waves of the surveys.12 ,13 While the self-report measure in the BCS appeared to be more accurate, with around 22% of self-identified ‘lifetime abstainers’ at 34 years drinking in the past survey, there may be a validity issue with this self-report measure; thus, we also use a bottom-up approach by taking consistent “Never nowadays” answers in successive waves as a different measure of being a persistent non-drinker. The percentage of lifetime abstainers derived using the bottom-up approach ranged from 1% to 2.1% in the NCDS and BCS. This did not differ greatly from the proportion of self-identified ‘lifetime abstainers’ in the BCS at 30 (2.1%) and 34 years (2.2%).
Early health
In the NCDS, a local authority medical officer collected extensive data on the medical history of the participants when they were 16 years. Here a systematic examination was carried out on details of skin conditions, respiratory tract infections, and defects in the cardiovascular system, the alimentary tract, the urogenital system, hernias, bones and joints and the neuromuscular system. We converted each condition into a binary variable representing whether the condition was present (no disability to degree unknown) or not. We also created another binary variable to model whether a participant had at least one slight to severe disability or not.
Long-standing and limiting long-standing illness
Binary variables derived from yes/no answers to the question “Do you have any longstanding illness, disability or infirmity which limits your activities in any way compared with people of your own age?” were used to measure health status across different time waves by creating a four-category variable as was carried out with self-rated poor health in a different longitudinal study.14 At age 33, this included all those who did not have a limiting long-standing illness (LLSI) at ages 23 and 33 as the reference category. The other three categories included those who had an LLSI at age 23 but not at 33, those who had an LLSI at age 33 but not at age 23, and finally all those who had an LLSI in both waves. To combine LLSI information from ages 23, 33 and 42, we reduced the three binary variables to four categories to keep the degrees of freedom within the model. This includes two categories, one with participants who did not have an LLSI at age 42 but had an LLSI at age 23 or 33, and the other with participants who had an LLSI at age 42 who may or may not have had an LLSI at age 23 or 33. The reference and the final categories are those that did not have an LLSI and had an LLSI in successive waves, respectively.
The same variable derivation was applied to the BCS at ages 26, 30 and 34; however, with long-standing illness (LSI), as it was asked consistently in each wave (in the NCDS, only LLSI was asked consistently), LSI was derived through yes responses to the question “Do you have any long-standing illness, disability or infirmity? By long-standing, I mean anything that has troubled you over a period of time?” There is substantial overlap between LLSI and LSI, with LLSI illness questions often being asked only of respondents who said yes to having an LSI. In the NCDS, for example, 65.4% of respondents with an LSI said that this was a LLSI at 33 years when both questions were asked.
Controls
All models were adjusted for self-report measures of sex, highest qualification, marital status, children under 16 years in the household and poor psychosocial health. Poor psychosocial health was derived from ‘yes’ answers to the Malaise Inventory, which has been found to be a valid measurement of psychosocial health,15 using the full 24 item scale categorised into normal (0-7) and high (8-24).15 At age 34 in the BCS, only 9 of the original 24 items were asked, resulting in a 4+ cut-off for depression. We used the most recent responses at the corresponding age of the model in both cohorts. For example, for lifetime abstainers’ age 33 in the NCDS, we used the highest qualification as recorded at age 33.
Statistical analysis
χ2 Tests were carried out on items from the medical examination at age 16 by drinking status at age 23 in the NCDS to observe whether each medical problem at an earlier age had a bivariate association with drinking in young adulthood.
Logistic regression on the odds of being a lifetime abstainer is used to explore whether remaining in ill health is associated with remaining a non-drinker, by examining associations with LLSI or LSI status between waves in the NCDS and BCS, adjusting for sex, Malaise Inventory score, highest qualification, marital status and children in the household, recorded in the most recent survey at the corresponding age of the model.
Results
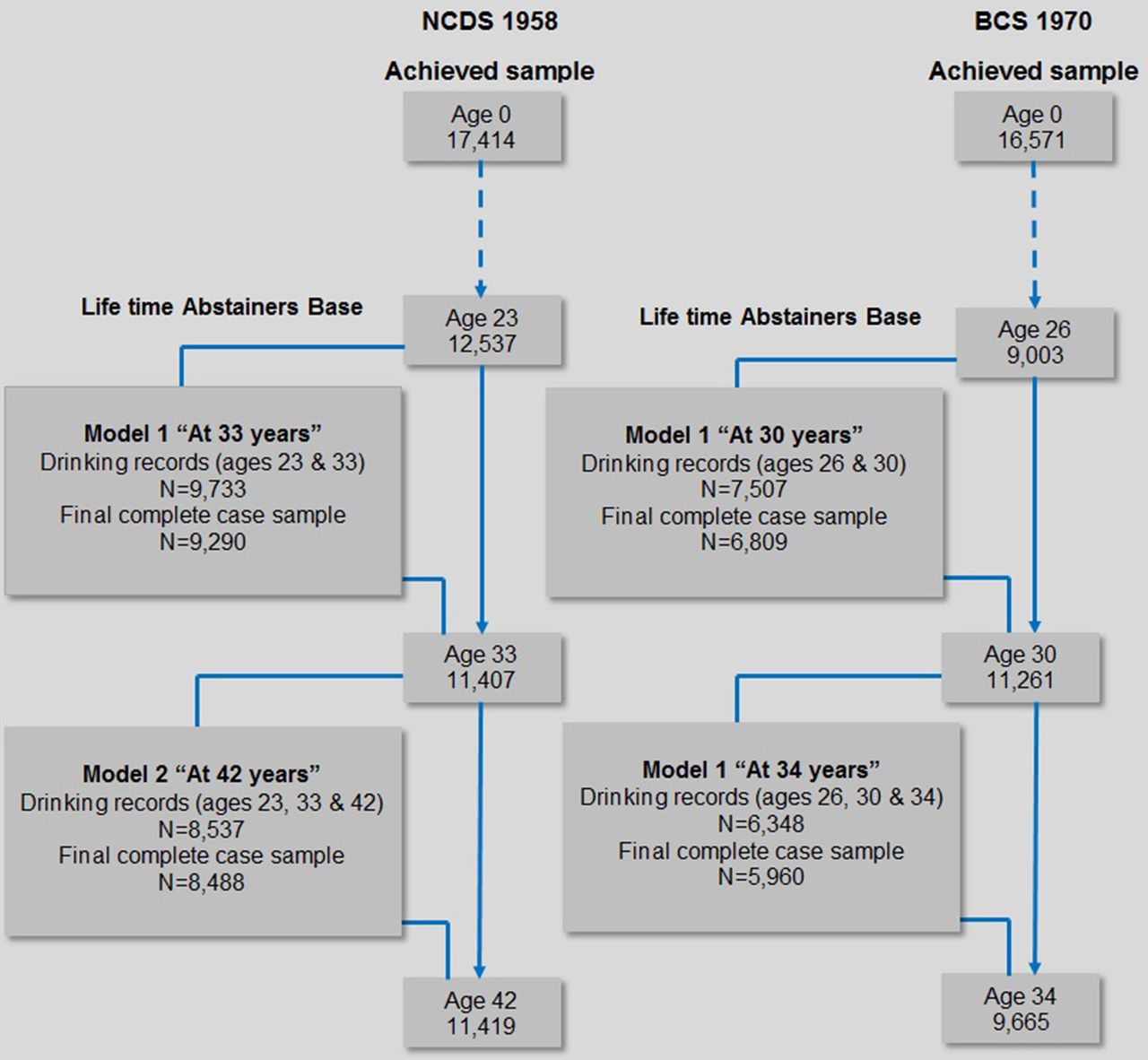
Figure 1 shows the sample achieved at each wave. In the NCDS, taking age 23 as the baseline for analysis, around 77.6% of respondents had drinking records at ages 23 and 33 and 68.1% up to age 43. In the BCS, around 83.4% of those with drinking records at age 26 had records at age 30 and 70.5% up to age 34. The BCS suffered from greater attrition than the NCDS, particularly at age 26, where participants had to opt in by sending through a postal questionnaire. Complete cases were not lower than 90% of those with drinking records at consecutive waves.
{kind=link}
Sample base from the National Child Development Study (NCDS) 1958 and British Cohort Study (BCS) 1970 used in logistic regression models.
Rates of earlier health conditions with drinking status in the NCDS and BCS
In the NCDS in table 1, around 82.2% of respondents with drinking records at age 23 had medical records at age 16 and this did not appear to differ significantly by drinking group (table 1). Where there was a statistical difference between drinking status and rates of conditions, non-drinkers had the highest rates of speech (5.7%), mental disability (9.8%), emotional and behavioural problems (6.5%), physical disability (9.5%), epilepsy (2.4%), heart (3.2%) and other central nervous system conditions (2.1%).
Percentage rates of medical conditions at age 16 assessed by a medical officer by drinking status at age 23 in the National Child Development Study 1958
Changes in LLSI and persistent non-drinking from age 23 in the NCDS
In table 2, using the NCDS, those who had an LLSI in successive waves from age 23 had 4.50 times the odds (95% CI 1.99 to 10.18, p<0.001) of being a lifetime abstainer at age 33 and 7.02 times the odds (2.39 to 20.66, p<0.001) at age 42, adjusting for all factors. In addition, having an LLSI in at least one wave before the age of the model since age 23 was positively associated with being a lifetime abstainer at age 33 (1.57 to 5.08, p<0.001) and 42 (1.73 to 5.77, p<0.001). Currently having an LLSI, whether the respondent had one previously or not, was associated with being a lifetime abstainer at age 42 only (1.33 to 3.45, p<0.01). People who were separated and divorced at age 33 were less likely than those who were single to have been a lifetime abstainer (0.23 to 0.99, p<0.05). Women were statistically significantly more likely to be lifetime abstainers in every model (p<0.001).
OR of being a lifetime abstainer (n)* and changes in limiting long-standing illness adjusted for all variables in the model taken at the corresponding age of analyses, in the National Child Development Study 1958
Changes in LSI and persistent non-drinking from age 26 in the BCS
In table 3, using the BCS, people who had an LSI in all time waves since age 26 had 2.80 times (1.88 to 4.18, p<0.001) the odds of someone who never had an LSI of being a lifetime abstainer at age 30, and 3.33 times the odds (2.01 to 5.53, p<0.001) at age 34, while adjusting for all factors.
OR of being a lifetime abstainer (n)* and changes in long-standing illness adjusted for all variables in the model taken at the corresponding age of analyses, in the British Cohort Study 1970
Changes in LSI and self-identified ‘lifetime abstainers’ from age 30 in the BCS
Similarly for self-identified ‘lifetime abstainers’ who are those who reported “never had an alcoholic” in table 4, those who had an LSI in all waves had 2.11 times (1.24 to 3.57, p<0.01) the odds of someone who never had an LSI of being a self-identified ‘lifetime abstainer’ at age 30 and 2.80 times the odds at age 34 (1.62 to 4.84, p<0.01). Having previously had an LSI but not currently was also significantly associated with being a self-identified ‘lifetime abstainer’ at age 30 (OR 2.07, 1.08 to 3.98; p<0.05) and 34 (OR 2.02, 1.20 to 3.42; p<0.001). Having children was also associated at age 30 (OR 1.89, 1.21 to 2.97; p<0.01). Gender had no effect in each of the BCS models.
OR of being a self-identified ‘lifetime abstainer’ (n) and changes in long-standing illness since age 26, adjusted for all variables in the model taken at the corresponding age of analyses, The British Cohort Study 1970
Discussion
Non-drinkers have been found to have higher rates of self-reported illness in young adulthood10 ,11; however, this is the first paper to show that objectively assessed medical conditions at 16 years were more common among non-drinkers in their 20s. Furthermore, people who reported having a self-reported illness over consecutive waves were more likely to have remained non-drinkers over the same time waves. This was the case for LLSI in the NCDS from 23 to 42 years and LSI in the BCS from 26 to 34 years. Consistent evidence between cohorts provides strong support that ill health is associated with continued non-drinking at different stages of the life course, particularly if the condition is persistent. Furthermore, an association with LSI and LLSI shows that it is not just people with severe illness or with disability who do not drink alcohol; however further analysis should be carried out on the effects of the severity of health condition on the consumption of alcohol within the same cohort.
We also found associations between persistent LSI and those who consistently stated that they were non-drinkers in each wave and participants who self-identified themselves as being lifetime abstainers in the BCS at 30 and 34 years, providing two different methods of deriving lifetime abstainers. This implies that illness is associated with those who consistently say that they are non-drinkers over time and those who claim to be lifetime abstainers. This has implications for either as a control group against drinkers, where the latter has already been found to be subject to validity issues, as those who claim to have never ever drunk alcohol were found to have reported drinking in previous surveys.12 ,13
Additionally, having previously had an LLSI but not having one currently was significantly associated with lifetime abstention in the NCDS as well as with self-identified ‘lifetime abstainers’ in the BCS, at each time point, which supports the argument that some people never ever take up drinking because of ill health from an early age. This may reflect people who never start drinking due to illness and continue to abstain even once health improves, particular when an earlier age of onset of drinking has been shown to be related to alcohol use in adulthood.16 Alternatively, a condition may have improved with medication; however, the continued use of medication prohibits the use of alcohol, or the condition may have been normalised over time so that the participant no longer see it as limiting. Unfortunately, we are unable to verify this with the dataset.
Evidence shows that non-drinkers have poorer psychosocial health than drinkers,17 ,18 including in early adulthood.10 ,19–21 It is possible that prior health conditions may be confounding the relationship between poorer mental health and non-drinking found in other studies as, to our knowledge, this is the first study to combine LSI and psychosocial health measured by the malaise inventory. In this study, however, while we controlled for a measure of psychosocial health, we cannot rule out that mental health may actually be an LLSI, although LLSI has been found to have stronger associations with physical functioning than mental and social well-being,22 ,23 while another study using the NCDS found that the stability of LLSI in early adulthood across a decade was associated with prior diagnoses of disability in childhood.23
The reasons why poor health has been found to be associated with non-drinking in this study and others8 ,9 ,11 may be due to the direct impact of drinking on the health condition or interference with medication. Many medications interact harmfully with the consumption of alcohol, prohibiting the use of alcohol, including medications for epilepsy and muscular pain24 ailments, which were found to be more common among non-drinkers in early adulthood (table 1). This may be the reason for the presence of associations of poor health and non-drinking across the life course, as we found in this study, and may also be a contributory factor towards the sick-quitter phenomenon. Another important consideration is the social gradient in non-drinking where people with lower incomes and less education are more likely to be non-drinkers.11 ,25–27 Low social economic status, poor health and mental health all interrelate and contribute to disadvantage and deprivation, resulting in higher morbidity, and may suggest interdependent and indirect effects of each on non-drinking through social exclusion.
Rates of lifetime abstainers did not differ greatly between cohorts, which may represent a stable and steady group among the drinking population. Women were more likely to be lifetime abstainers in every regression model in the NCDS; however, among the younger cohort in the BCS, gender had no effect. This may be a consequence of more acceptable drinking norms for women where drinking rates have risen among women over the past decades. Unfortunately, owing to the low sample size of lifetime abstainers, we were unable to stratify by gender. For future studies, the effects of health on drinking should be assessed in populations where drinking is less of a norm. In such populations, we imagine the effect of health to be lower among non-drinkers due to the higher number of ‘average’ people among non-drinkers where drinking is less normative.
The strengths of the study include the use of two large nationally representative cohort studies and finding consistent results, particularly with the association between persistent LLSI and LSI and remaining a non-drinker over time. The limitations of this paper include missing data. Since we used complete case analysis that depended on data from consecutive waves, there was a large proportion of missing data, largely attributable to attrition (figure 1). We find no statistical variation between missing data at age 23 and medical records at age 16 in the NCDS (table 1) and consistent findings between two cohorts. We also cannot rule out an element of missing not at random when concerning LLSI as some may have been too ill to participate in the next wave. However, if our hypothesis that non-drinking is a consequence of poor health is true, then this would underestimate the associations due to a reduced sample from people who were very ill; however, we were unable to verify this.
Conclusion
The existing health problems from earlier life or chronic health problems during adulthood may influence why some people never ever drink alcohol. Even lifetime abstainers may suffer from pre-existing poor health, and therefore the better health outcomes of moderate drinkers compared with non-drinkers may be subject to bias. Care should be taken in verifying the previous and existing health status of drinking groups in studies which aim to examine the short-term or long-term effects of alcohol on adult health.
What is already known on this subject
-
A J-shaped relationship is observed between alcohol consumption and mortality outcomes with moderate drinkers having better health and mortality outcomes than non-drinkers.
-
Lifetime abstainers have been used as a reference group to eliminate bias that may arise from including ex-drinkers who have stopped drinking due to worse health.
-
It is not known whether poor health from an early age or ongoing poor health may be a reason why some people never ever take up drinking.
What this study adds
-
Objectively assessed medical conditions at age 16 were higher among non-drinkers in early adulthood.
-
Having a limiting long-standing illness or long-standing illness consistently across adulthood is a predictor of being a lifetime abstainer independent of social, demographic and psychosocial health factors.
-
Illness from an early age and ongoing illness may be a reason why some never ever take up drinking alcohol. Studies which compare the health of moderate drinkers with lifetime abstainers may be subject to a pre-existing poor health bias.
References
Footnotes
-
Contributors LNF and NS had the original idea for the study. LNF, NS and NC developed the study design. LNF conducted all analyses and wrote the first draft. NC, MM and NS advised on the statistical aspects of the study design, analysis stages and revision of drafts, and were involved in the discussion and interpretation of results. LNF is the guarantor for the study.
-
Competing interests Alcohol Research UK (ARUK) and UCL Impact provided a scholarship to fund LNF's PhD.
-
Ethics approval Ethical approval was obtained from relevant approval bodies in the UK at the time of data collection. Access to the dataset for the purposes of secondary analysis was subject to the terms of an end-user license agreement, and further ethical approval was not needed.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The technical appendix and statistical code are available from LNF at l.ngfat.10@ucl.ac.uk. The data are available from the Economic and Social Data Service (http://www.esds.ac.uk) subject to an end-user license agreement.
Linked Articles
- Corrections